Role: Evidence Lead & Content Development Designer | Timeline: Sept 2024 – Dec 2025 | Status: Delivered
Overview
A global pharmaceutical company needed to unify its patient support programs for insulin therapy. Each country in its network had developed its own version of the program independently, and the result was a patchwork: inconsistent structures, inconsistent evidence bases, and no shared standard for what patients should know. The company wanted a single core curriculum that could be deployed across dozens of international markets, with room for regional supplemental content where local clinical practices or regulations required it.
This case study describes how I built an internationally grounded evidence framework, developed a structured content production process, and shepherded the resulting materials through cross-geography regulatory review.
Client and Context
The pharmaceutical company had been offering managed patient support programs for insulin therapy patients across its international markets. The programs helped patients manage type 2 diabetes through education, lifestyle guidance, and ongoing support. Each country had built its own version, and the programs varied in depth, clinical accuracy, and educational approach.
The company engaged a digital health content team through a technology vendor that was building a web application to house the unified program. The content team was responsible for creating the educational materials: the core curriculum shared across all markets, plus an initial regional supplement for the first launch market in Europe.
The Problem
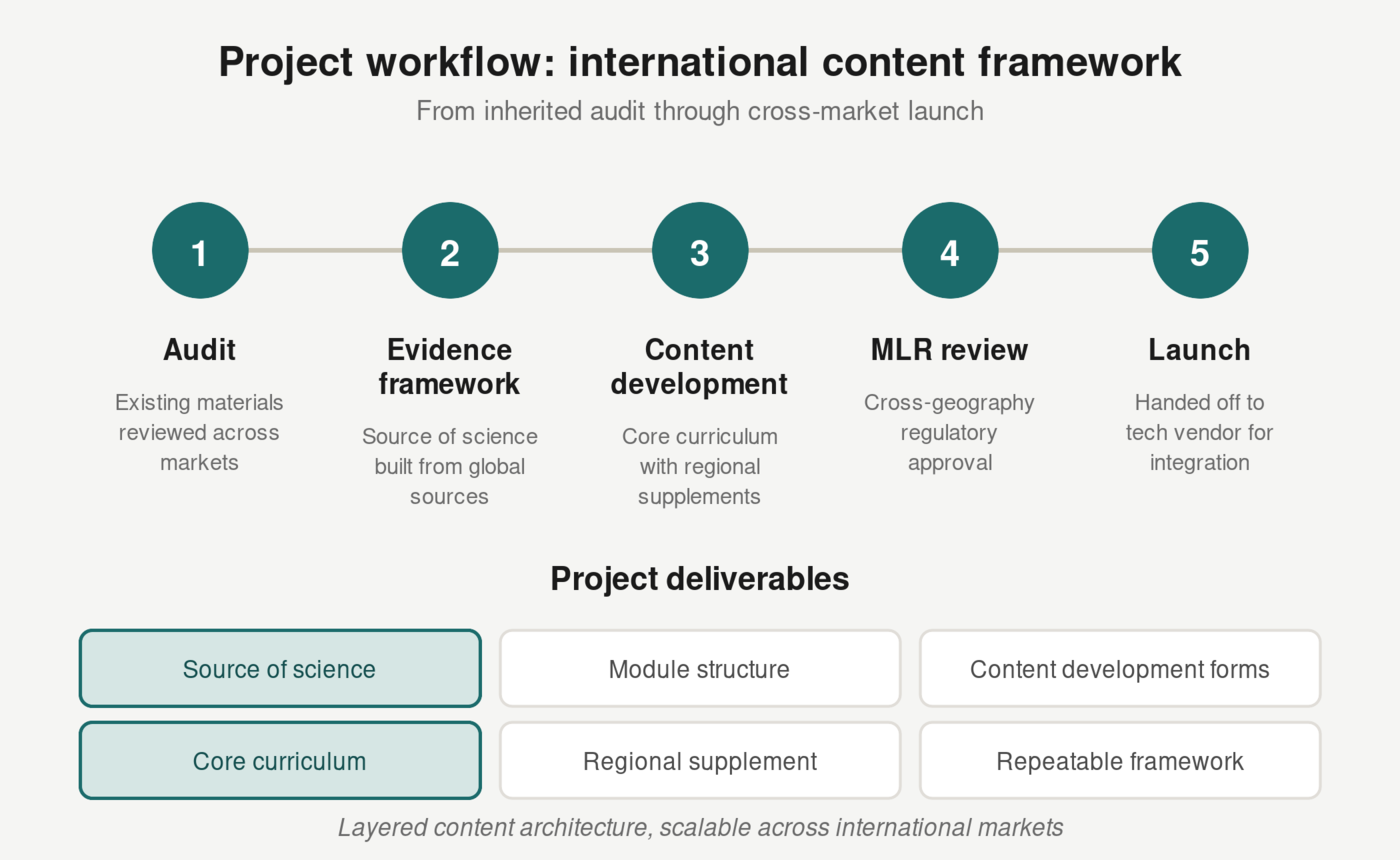
An initial audit of five countries’ existing program materials revealed significant inconsistencies: gaps in key education topics, variable approaches to the same clinical concepts, inconsistent tone, and out-of-date content still in active circulation. A colleague completed this audit and developed the first content framework, designating which topics belonged in the universal core curriculum and which were appropriate as regional supplemental content. That work established the structural foundation for the project.
After the audit was complete, the project transitioned to me. I inherited the framework and the core-versus-supplemental designations, and was responsible for evidence sourcing, content development, and regulatory review from that point forward.
Three structural challenges shaped the work ahead.
International evidence sourcing. The content couldn’t rely on a single country’s clinical guidelines. Recommendations grounded in one national context would lack applicability in other markets. The evidence base needed to draw from internationally recognized sources so that core recommendations held up regardless of where the program launched.
Cross-geography regulatory review. The MLR board operated out of a different region than the client contacts and the first launch market. Time zone differences, communication delays, and differing expectations about acceptable content meant that feedback cycles stretched into weeks.
Designing for adaptation. The core content needed to be specific enough to be useful to patients, but structured so that individual markets could modify or supplement it based on local practices, regulations, and cultural context. Content that was too specific to one country’s context would need to be created from scratch for another, rather than adapted.
The Approach
Inherited foundation
A colleague audited the existing materials from multiple countries, assessed what each market’s program covered, identified gaps and overlaps, and developed recommendations for the unified core curriculum. This audit established the module structure: which topics were universal, which were market-specific, and how the two layers should relate to each other. I inherited this framework when the project transitioned to me.
Evidence framework
With the module structure in hand, I built the evidence base that would anchor every piece of content in the program: the “source of science.”
The sourcing methodology had to account for the international scope. Instead of relying on guidelines from any single country’s health authority, I drew from internationally recognized bodies and research organizations: global diabetes federations, multinational clinical research, and cross-border public health guidance. Every recommendation was linked to its supporting evidence, creating a traceable chain from clinical literature to patient-facing content. The source of science was a living document; it was revised and expanded throughout the project as MLR feedback and scope changes from the client required updates.
The source of science also served a regulatory function. When MLR reviewers questioned a claim, I could point to the specific evidence behind it. This shifted review conversations from “can you say this?” to “here’s the evidence,” which reduced the number of rounds needed to reach approval.
Content development
With the evidence framework in place, I built content development forms for each module. These forms documented the structure, key education points, and evidence citations for every piece of content in the program. They served as the blueprint that guided the production studio (graphic design, copywriting, editorial, videography, animation), keeping every asset aligned with the evidence base.
This was largely a fresh build. While legacy files from the client’s existing programs were referenced to understand how the coaching program was structured overall, the educational content, coaching call guides, and FAQs were created from scratch. The inherited framework and core-versus-supplemental designations shifted over the life of the project as the client and end customer provided input and scope evolved.
Each piece of content went through MLR review. The team and I incorporated feedback, resubmitted revised versions, and handed approved versions off to production. This process repeated for every piece of content in the core curriculum and the initial regional supplement.
The Core Design Challenge
The central tension was building content that was specific enough to be useful to patients, while structured in a way that could work across countries.
Insulin therapy involves universal concepts: blood glucose monitoring, injection technique, hypoglycemia management, lifestyle adjustment. But the specifics vary by market. Different countries have different standard care practices, different measurement units, different dietary norms, and different healthcare system structures that shape how patients interact with their care teams.
The solution was a layered content architecture. The core curriculum covered the universal fundamentals, anchored in internationally sourced evidence. Regional supplements covered market-specific practices, cultural considerations, and local regulatory requirements. The two layers were designed to read as a single program from the patient’s perspective.
Regulatory Review Across Geographies
The MLR review process was complicated by geography. The review board, the client contacts, and the first launch market were in different regions. Every review cycle involved time zone gaps, communication chains that passed through multiple stakeholders, and differing expectations about what constituted acceptable content.
My approach was to front-load the evidence work. By building a cited source of science before drafting any patient-facing content, I grounded every MLR conversation in documented evidence. When a reviewer flagged a concern, the response was a citation and a rationale. This didn’t eliminate the friction of cross-geography review, but it reduced the number of rounds needed and kept conversations focused on the content itself.
Outcome
The core content framework was completed and approved through MLR review. The source of science, module structure, and content development forms were delivered to the technology vendor for integration into the digital platform. The initial regional supplement for the first European launch market was also completed.
The framework gave the client a repeatable process for scaling: each new market would adopt the core curriculum and develop its own supplement using the same methodology and content development process. The digital platform and broader rollout are ongoing.
Lessons and Implications
International evidence sourcing requires a deliberate methodology. Building a credible evidence base for international content means identifying which sources carry authority across markets, mapping where national guidelines converge and diverge, and deciding what to anchor in universal evidence versus what to defer to local adaptation. For this project, the source of science functioned as both a clinical reference and a regulatory tool.
Specificity and structure makes content adaptable. The core curriculum had to be precise about what it covered, how it was structured, and what evidence supported each component. Downstream teams in other markets would need to make informed decisions about what to keep, adapt, or supplement. Content without clear structure and evidence grounding can’t be meaningfully evaluated or built upon by another team.
The evidence library is not a strategy; it’s a regulatory requirement. MLR boards require clear documentation linking every claim to its source. The evidence base has to exist before content development begins; there is no shortcut around this. On this project, the client initially underestimated how rigorous that documentation needed to be and how much time the process would take. Part of the work was helping the client understand that evidence sourcing isn’t a phase you can compress; it’s the foundation that determines how smoothly everything after it goes.
Build real time into the timeline for MLR. Cross-geography regulatory review is slow, and it should be. MLR boards exist to protect patients, and that means they will flag things that don’t have clear support, even when the reasoning behind the content seems obvious to the team that wrote it. Reviewers will sometimes come back with feedback that doesn’t track with the content team’s logic, and that’s part of the process. Timelines need to account for this. On this project, the gap between the client’s expected timeline and the reality of multi-region MLR review was significant. Building in adequate buffer for unexpected review cycles isn’t a nice-to-have; it’s a project planning requirement.